Why It Is So Common
Across veterinary-clinic populations of adult dogs, periodontal disease at some stage is the most prevalent single clinical finding. The widely-quoted "80 percent of dogs over 3" figure comes from clinic populations rather than a clean random sample, but the qualitative claim — most adult dogs have measurable periodontal disease — is robust across studies.
The reason is the same combination of factors that produces dental disease in any species: the oral cavity is a warm, moist, nutrient-rich environment that supports a polymicrobial biofilm; mechanical disruption of that biofilm is the only thing that prevents progression; and unlike humans, dogs do not perform that disruption themselves. Without owner-delivered or vet-delivered intervention, plaque accumulates at the gum line, mineralises into calculus, and the host immune response to subgingival bacteria does the rest. Niemiec's 2008 review remains the standard practitioner reference for the pathophysiology and clinical staging[^niemiec2008].
The Pathophysiological Cascade
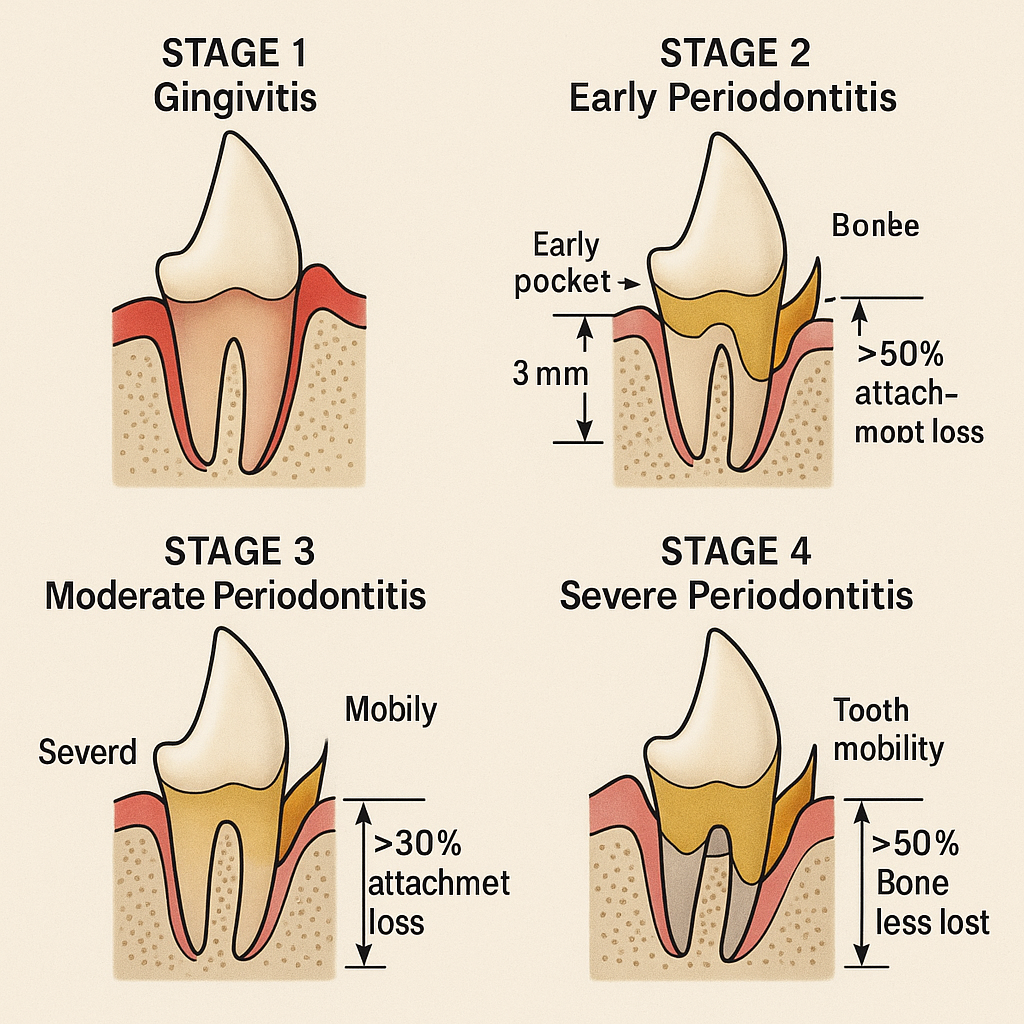
The progression has discrete stages, and the clinical interventions differ by stage:
- Stage 1: gingivitis. Inflammation confined to the gum margin. Reversible with thorough plaque control. Visible signs: red, swollen gum line, possibly mild bad breath.
- Stage 2: early periodontitis. Up to 25 percent attachment loss; small periodontal pockets. Beginning of bone involvement; not fully reversible but stoppable with professional cleaning plus consistent home care.
- Stage 3: moderate periodontitis. 25-50 percent attachment loss; deeper pockets; clinical mobility may begin. Requires professional intervention with localised periodontal therapy.
- Stage 4: severe / advanced periodontitis. >50 percent attachment loss; furcation involvement; tooth mobility; often extraction is the appropriate treatment.
Crucially, all of this happens below the gum line. The visible-from-above tooth surface is a poor indicator of subgingival disease, which is why staging requires probing and dental radiographs under anaesthesia.
The Oral-Systemic Link
The argument that "dental disease is a whole-dog problem" is sometimes overstated in pet marketing, but the underlying evidence base in dogs is real for some endpoints. Glickman and colleagues' 2009 JAVMA analysis is the cleanest demonstration: in a large insured-dog cohort, severity of periodontal disease was associated with increased risk of cardiovascular endpoints (endocarditis, cardiomyopathy) in dose-dependent fashion[^glickman2009]. The proposed mechanism — repeated bacteraemic episodes from inflamed periodontal pockets, with selective binding of oral Streptococcus and other species to cardiac valves — is the same one established in human cardiology.
Pavlica and colleagues' (2008) histopathological work documented inflammatory changes in distant organs correlated with periodontal-disease burden in dogs[^pavlica2008]. The renal and hepatic links are biologically plausible and suggestive in published case-series, though less cleanly established than the cardiovascular case.
The honest framing for owners: periodontal disease is at minimum a quality-of-life problem (chronic oral pain is meaningful even if the dog does not show it dramatically), and in moderate-to-severe form is associated with measurable systemic-disease risk.
What Actually Prevents It

The interventions that work are mechanical disruption of plaque before it mineralises:
- Daily tooth brushing with a canine enzymatic toothpaste is the gold standard. The daily qualifier matters: plaque mineralises into calculus over 24-72 hours, and brushing every-other-day or three times a week is appreciably less effective. Use a soft-bristled brush or finger brush; never use human toothpaste (fluoride and xylitol are toxic to dogs).
- VOHC-accepted dental chews and diets. The Veterinary Oral Health Council maintains a list of products with documented efficacy in plaque or calculus reduction. The acceptance is not a marketing seal; it requires submitted study data. VOHC-accepted chews are a useful adjunct but not a replacement for brushing.
- Water additives and dental sprays with VOHC acceptance can produce small additional reductions. Reasonable adjunct, not a primary intervention.
- Diet texture matters less than the marketing implies. Hard kibble produces small reductions in calculus accumulation versus wet food at the dental-surface level, but the magnitude is much smaller than brushing achieves.
The intervention that does not work and is explicitly cautioned against by the American Veterinary Dental College is "anaesthesia-free dental cleaning" — typically scaling visible calculus on an awake dog. It addresses cosmetics, not disease, because the disease is subgingival and cannot be safely or thoroughly addressed without anaesthesia.
Professional Cleaning
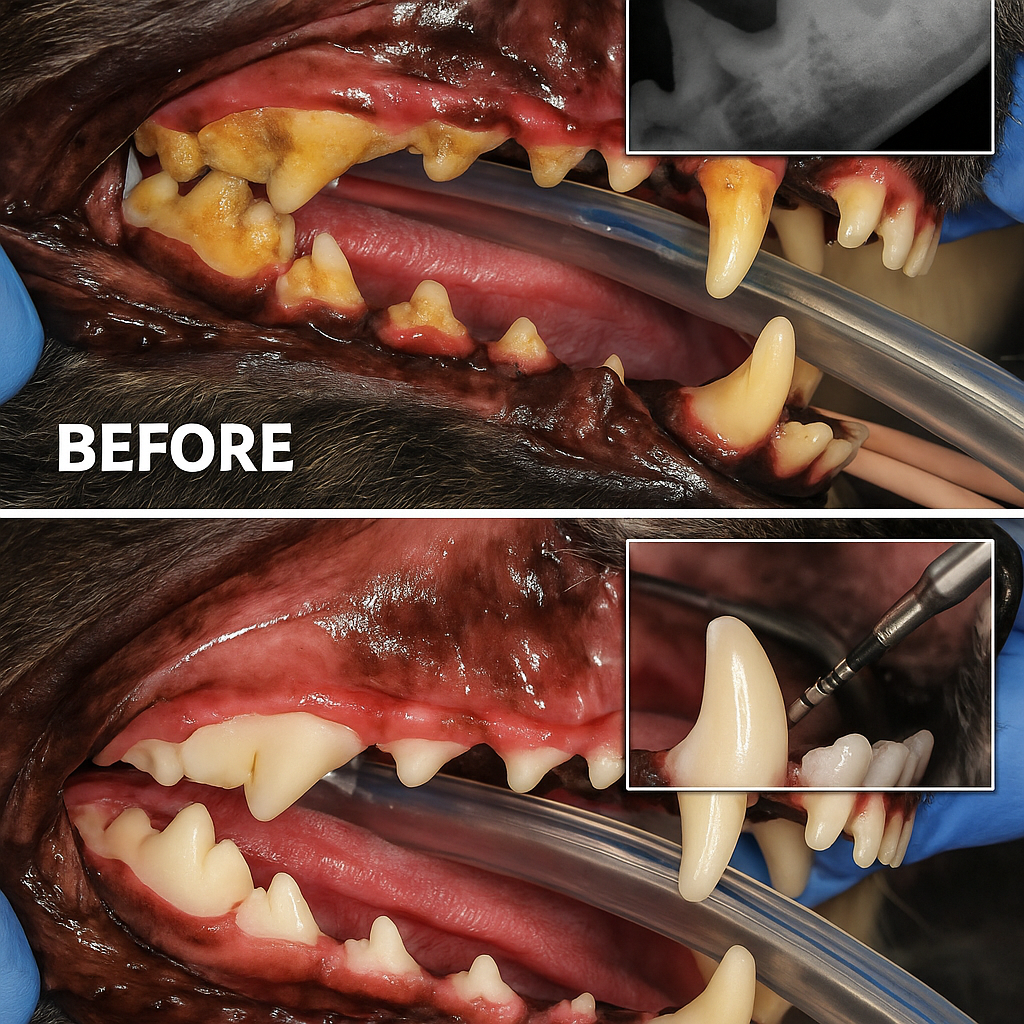
A complete oral health assessment and treatment (COHAT) under general anaesthesia is the only way to fully evaluate and treat subgingival disease. The components: full-mouth dental radiographs (without which much of the disease is invisible), probing, scaling above and below the gum line, polishing, and any indicated extractions or periodontal therapy.
The AAHA 2019 Dental Care Guidelines are the contemporary practitioner reference for the protocol[^aaha2019]. The interval depends on the dog: small-breed and brachycephalic dogs (more crowded dentition) typically need annual cleanings; medium-to-large breeds without active disease can often go longer; dogs with established disease are on a shorter cycle.
The anaesthesia question owners ask: modern protocols with appropriate pre-anaesthetic bloodwork, multimodal anaesthesia, and continuous monitoring are very low-risk in healthy adult dogs. Avoiding necessary dental care to avoid anaesthesia exposes the dog to the larger risk of progressive periodontal disease.
What Is and Is Not Settled
Settled: high prevalence of periodontal disease in adult dogs (Niemiec 2008); cardiovascular-disease association with periodontal-disease severity (Glickman 2009); efficacy of daily mechanical plaque disruption; necessity of anaesthesia for thorough subgingival assessment and treatment.
Not settled: the magnitude of renal and hepatic risk attributable to periodontal disease; the comparative efficacy of various VOHC-accepted products at population scale.
Key Takeaways
- Most adult dogs have measurable periodontal disease; the disease lives subgingivally and is invisible from above the gum line.
- Daily tooth brushing with canine enzymatic toothpaste is the gold-standard prevention.
- VOHC-accepted chews and water additives are useful adjuncts; "anaesthesia-free cleaning" is cosmetic, not therapeutic.
- Periodontal-disease severity is associated with cardiovascular endpoints in dogs (Glickman 2009).
- Professional cleaning under general anaesthesia is the only way to assess and treat the actual disease (AAHA 2019 guidelines).
Sources & further reading
- Niemiec, B. A.. (2008). Periodontal disease. Topics in Companion Animal Medicine, 23(2), 72-80. https://doi.org/10.1053/j.tcam.2008.02.003
- Glickman, L. T.; Glickman, N. W.; Moore, G. E.; Goldstein, G. S.; Lewis, H. B.. (2009). Evaluation of the risk of endocarditis and other cardiovascular events on the basis of the severity of periodontal disease in dogs. Journal of the American Veterinary Medical Association, 234(4), 486-494. https://doi.org/10.2460/javma.234.4.486
- Pavlica, Z.; Petelin, M.; Juntes, P.; Eržen, D.; Crossley, D. A.; Skalerič, U.. (2008). Periodontal disease burden and pathological changes in organs of dogs. Journal of Veterinary Dentistry, 25(2), 97-105. https://doi.org/10.1177/089875640802500210
- Bellows, J.; Berg, M. L.; Dennis, S.; Harvey, R.; Lobprise, H. B.; Snyder, C. J.; Stone, A. E. S.; Van de Wetering, A. G.. (2019). 2019 AAHA Dental Care Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association, 55(2), 49-69. https://doi.org/10.5326/JAAHA-MS-6933
- Niemiec, B.; Gawor, J.; Nemec, A.; Clarke, D.; McLeod, K.; Tutt, C.; Gioso, M.; Steagall, P. V.; Chandler, M.; Morgenegg, G.; Jouppi, R.. (2020). World Small Animal Veterinary Association Global Dental Guidelines. Journal of Small Animal Practice, 61(7), 395-403. https://doi.org/10.1111/jsap.13219