What Parvovirus Is
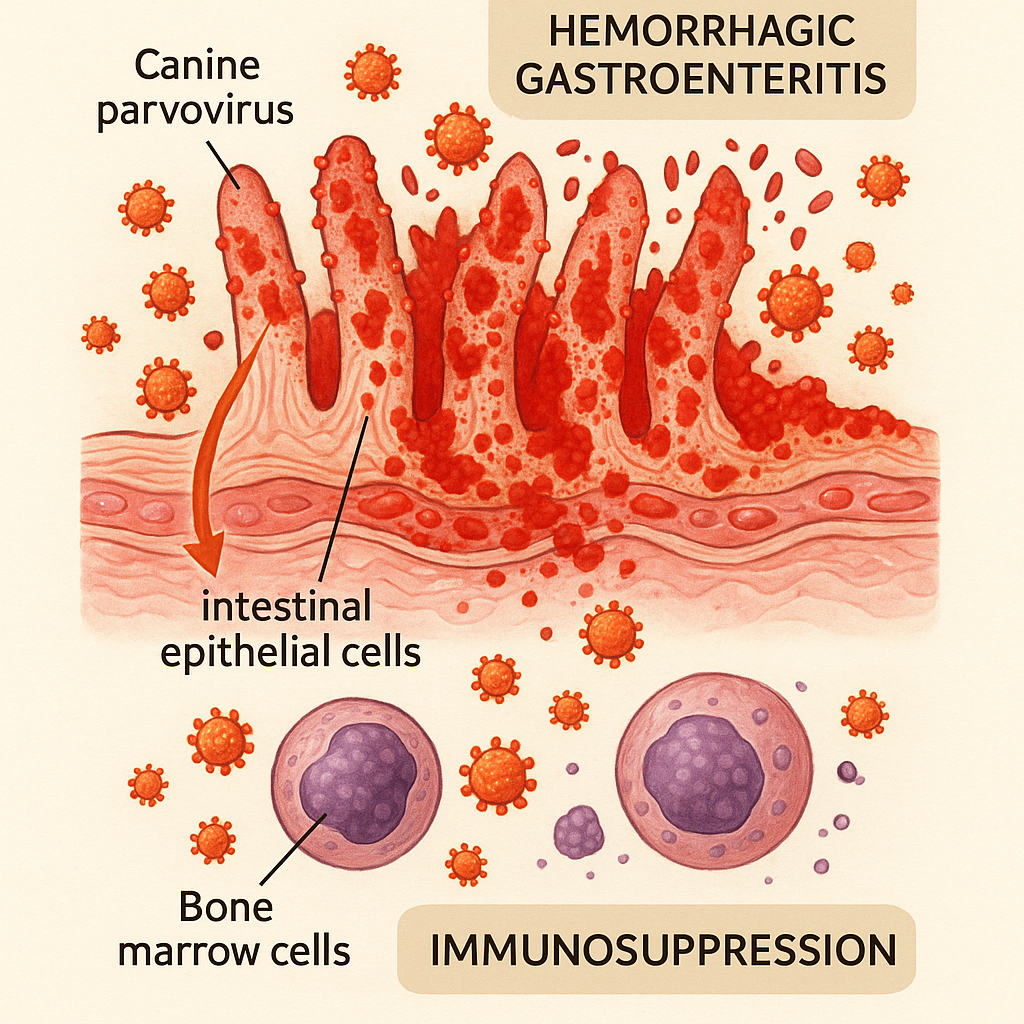
Canine parvovirus (CPV-2) is a small, non-enveloped DNA virus that emerged in the late 1970s and has since become one of the most significant infectious diseases of dogs worldwide. The virus targets rapidly-dividing cells, primarily the intestinal epithelial cells lining the small intestine and the bone marrow precursor cells of the immune system. The clinical syndrome reflects this targeting:
- Severe hemorrhagic gastroenteritis. Profuse vomiting, severe diarrhea (often bloody), severe dehydration, electrolyte disturbances.
- Immunosuppression. Bone marrow effects produce neutropenia (low white blood cell count), making secondary bacterial infections from gut translocation a major complication.
- Sepsis. The combination of compromised gut barrier and immunosuppression frequently leads to systemic bacterial infection.
Without treatment, mortality is high — historically 70-90% in untreated puppies. With aggressive modern hospitalised supportive care, survival rates of 70-90% are reasonable.
The virus is extraordinarily contagious. A single gram of feces from an infected dog can contain enough virus to infect millions of susceptible dogs. The virus is shed in feces during the acute illness and for some weeks after recovery.
Why It Is Particularly Dangerous to Puppies
Two factors make young puppies the highest-risk population:
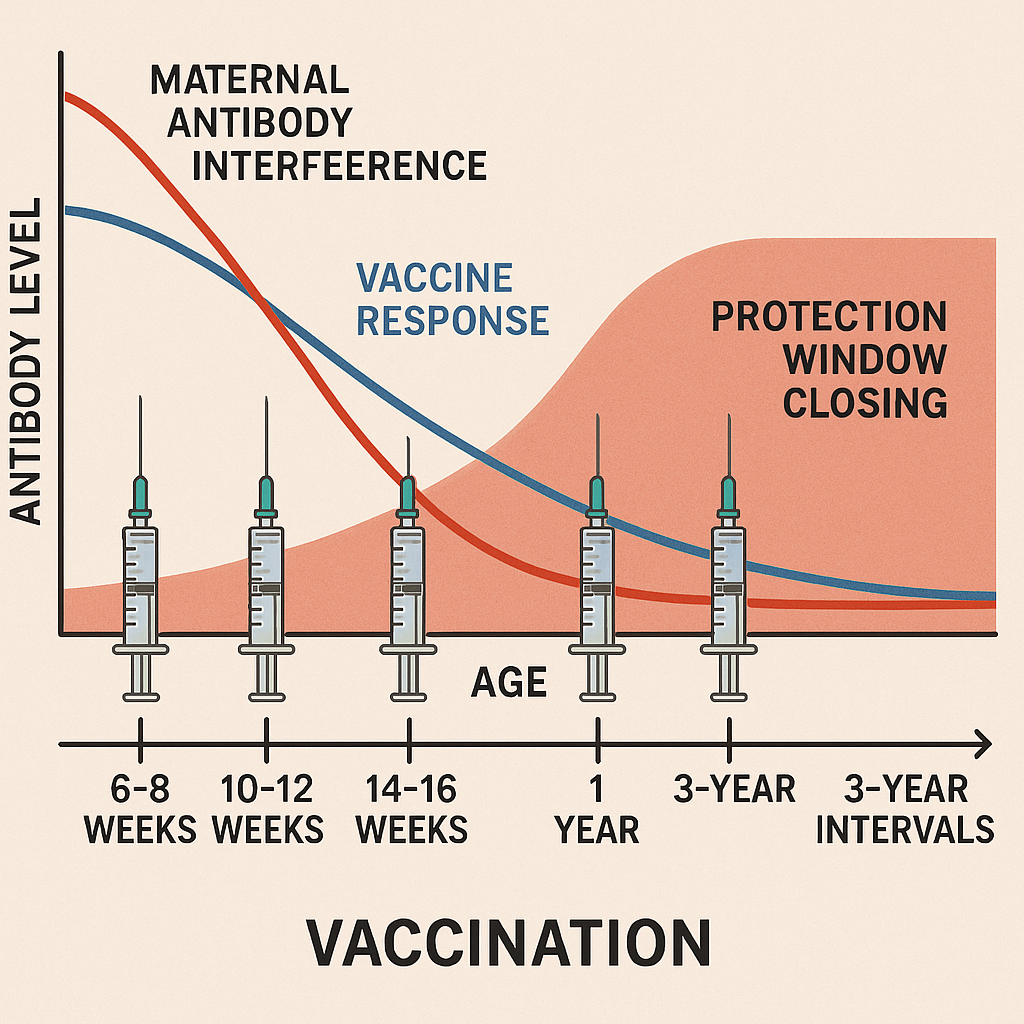
Maternal antibody interference and the "vaccine window". Puppies receive passive immunity from their mother through colostrum. Maternal antibodies provide protection during the early weeks but interfere with vaccine response — they neutralise the vaccine virus before the puppy's immune system can mount its own response. Maternal antibodies wane at variable times across individual puppies (typically 6-16 weeks). A puppy whose maternal antibodies have waned but who has not yet been successfully vaccinated has a vulnerable window. The standard approach to closing this window is the puppy series — multiple booster vaccines at 2-4 week intervals (typically 6-8 weeks, 10-12 weeks, 14-16 weeks) so that whenever the maternal-antibody window closes, a booster covers it.
Higher mortality in young animals. Puppies have less physiologic reserve to handle the dehydration, electrolyte disturbances, and sepsis of severe disease. Mortality in unvaccinated young puppies is appreciably higher than in older dogs.
Vaccination — The Primary Prevention
The WSAVA Vaccination Guidelines and AAHA Canine Vaccination Guidelines include parvovirus vaccine as a core vaccine — recommended for all dogs regardless of lifestyle or risk profile[^wsava][^aaha].
The standard puppy series:
- First vaccine: 6-8 weeks of age.
- Second vaccine: 10-12 weeks of age.
- Third vaccine: 14-16 weeks of age.
- Some protocols include a fourth at 18-20 weeks for high-risk environments or breeds known for prolonged maternal-antibody persistence (Rottweilers, Doberman Pinschers, some other breeds).
- First adult booster: 1 year after the puppy series.
- Subsequent boosters: every 3 years is the WSAVA recommendation; some practices use annually.
A puppy is not considered fully protected until at least 1-2 weeks after the final puppy-series booster. Until then, the puppy should be in low-risk environments — avoiding places where unvaccinated dogs have been (dog parks, pet stores, areas with stray-dog traffic, contaminated environments).
The socialization-vs-protection tension is real: the puppy socialization article covers this. AVSAB and the broader behaviour community support carefully-managed early socialization (in clean environments, with vaccinated dogs, in puppy classes that screen attendees) rather than complete isolation, despite the parvo risk.
Recognising Parvovirus
Classic clinical presentation in an unvaccinated or partially-vaccinated puppy:
- Lethargy and decreased appetite — often the first signs.
- Vomiting — typically severe and persistent.
- Diarrhea — often bloody, with characteristic foul odour.
- Severe dehydration — sunken eyes, dry mucous membranes, prolonged skin tent, weakness.
- Hypothermia in severe cases (rather than fever, late-stage parvovirus often produces low body temperature).
- Septic shock — collapse, weak pulse, altered mentation.
Diagnosis is typically by parvovirus antigen detection on a fecal sample using rapid in-clinic tests; PCR is more sensitive in some cases but the rapid antigen test is sensitive and specific enough for clinical decision-making in most cases.
Treatment
The standard approach is aggressive hospitalised supportive care:
- IV fluids — aggressive crystalloid fluid replacement, then maintenance plus ongoing-loss replacement.
- Antibiotics — broad-spectrum (typically ampicillin or cefazolin and an aminoglycoside or fluoroquinolone for gram-negative coverage) given systemically; the immunosuppression and gut barrier disruption produce frequent bacterial sepsis.
- Antiemetics — maropitant (Cerenia), ondansetron, or metoclopramide for vomiting control.
- Pain management — buprenorphine or other appropriate opioids; severe abdominal pain is part of the clinical syndrome.
- Nutritional support — early enteral feeding through nasoesophageal or nasogastric tubes when possible (improves outcomes vs. complete withholding of food until vomiting resolves).
- Plasma transfusion for severe hypoalbuminemia or coagulopathy in some cases.
- Antiviral therapy is limited; some practitioners use oseltamivir (Tamiflu) although evidence is mixed.
Hospitalised survival rates with modern supportive care are 70-90%. Some cost-constrained scenarios use outpatient protocols (subcutaneous fluids, oral antibiotics, antiemetics) with somewhat lower survival rates (estimated 60-80% in published outpatient series). Outpatient management is appropriate when hospitalisation is not financially feasible but is not as effective as hospitalised care.
Environmental Management
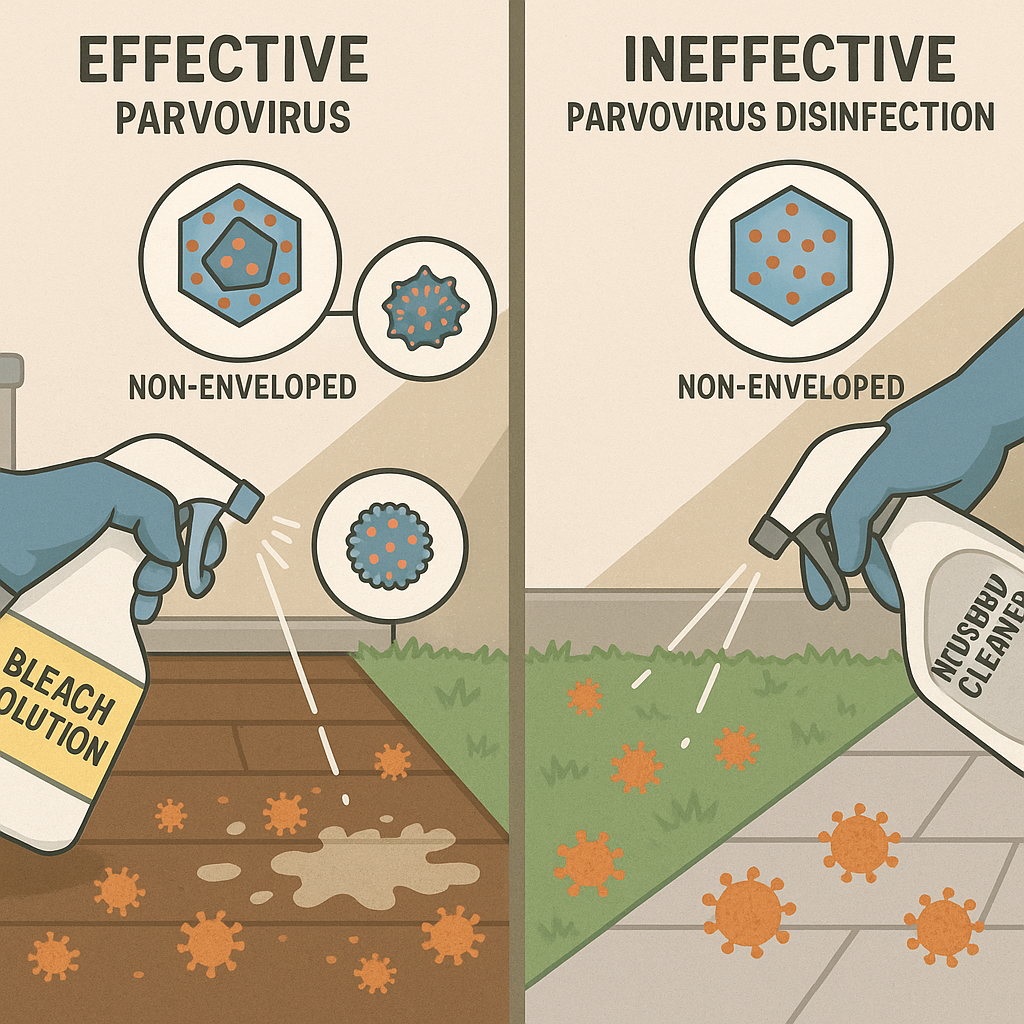
Parvovirus is one of the most environmentally persistent canine pathogens. The non-enveloped virus structure makes it resistant to:
- Most household cleaners.
- Many veterinary disinfectants.
- Heat (survives moderate temperatures).
- Drying.
- Time (remains infectious in soil for months to a year).
Effective decontamination requires:
- Bleach (sodium hypochlorite) at 1:30 dilution (about 1 part bleach to 30 parts water) — the standard parvovirus-effective concentration for surfaces. Allow 10+ minutes of contact time. Bleach is one of the few household chemicals reliably effective.
- Specific veterinary disinfectants with documented parvocidal activity (Rescue / Accel formulations, some others).
- Removing organic matter first — dirt and feces inactivate disinfectants; mechanical cleaning precedes disinfection.
- For yards and outdoor environments — chemical decontamination is not really feasible. Time (months) and weather are the typical decontamination process. Bringing a new puppy into a yard where a parvovirus puppy died is a real risk.
The implication: a household where a parvovirus puppy died should not introduce a new unvaccinated puppy until time has passed, surfaces have been thoroughly bleached, and any new dog has had their full vaccination series.
What This Does Not Imply
- The parvovirus vaccine is not 100% protective. It is highly effective but a small minority of fully-vaccinated dogs can still get parvo. The protection is substantial, not absolute.
- Survivors do not need ongoing parvo treatment. Recovered dogs are typically protected by natural immunity for life. They may shed virus for some weeks after recovery; isolation from other unvaccinated dogs is appropriate during that period.
- The vaccine causes parvo. Modified-live parvo vaccines do not cause clinical disease in healthy puppies.
What Is and Is Not Settled
Settled: parvovirus is a vaccine-preventable disease with effective vaccines included in the WSAVA and AAHA core vaccination protocols[^wsava][^aaha]; the puppy series at 6-8, 10-12, and 14-16 weeks closes the maternal-antibody-interference window; hospitalised supportive care produces 70-90% survival in modern protocols; environmental persistence is months to a year and bleach is the standard effective disinfectant.
Not settled: optimal antiviral and adjunctive therapies; the specific protocols that produce best outcomes in resource-constrained outpatient management; the role of newer monoclonal-antibody therapies (some research products in development).
Key Takeaways
- Parvovirus is highly contagious, environmentally persistent (months to a year), and severely deadly in untreated puppies.
- The vaccine is core — recommended for all dogs (WSAVA, AAHA).
- Standard puppy series: 6-8, 10-12, 14-16 weeks; adult booster at 1 year; resulting boosters every 3 years (WSAVA).
- Hospitalised supportive care produces 70-90% survival; outpatient protocols somewhat lower; without treatment, mortality is high.
- Environmental decontamination: bleach at 1:30 dilution with mechanical cleaning first; outdoor environments require time-and-weather rather than chemical decontamination.
- A puppy is not considered fully protected until 1-2 weeks after the final puppy-series booster.
Sources & further reading
- World Small Animal Veterinary Association. (2024). WSAVA Vaccination Guidelines for Dogs and Cats. World Small Animal Veterinary Association. https://wsava.org/global-guidelines/vaccination-guidelines/
- American Animal Hospital Association. (2022). AAHA Canine Vaccination Guidelines. American Animal Hospital Association. https://www.aaha.org/aaha-guidelines/vaccination-canine-configuration/
- American Veterinary Medical Association. AVMA Parvovirus Resources. American Veterinary Medical Association. https://www.avma.org/